

While many medical students diligently try to understand the mechanisms of disease in order to succeed on the USMLE Step 1, one of the hardest topics to do so is anemias. Specifically, connecting the mechanism of anemia with anything else – be it the MCV (mean corpuscular volume), the TIBC, or even the transferrin saturation levels, is a daunting challenge, one that has tripped up many a medical student. Here, by walking through the mechanism of anemia, we will be able to learn these topics to the depth I used to score a 270 on the USMLE Step 1. In addition to being able to connect the mechanism of anemia to MCV, by the end, you will be able to answer the following questions:
- Anemia of chronic disease – use mechanism of disease to explain iron panel results (TIBC, ferritin, transferrin sat, serum iron)
- Iron-deficiency anemia – use mechanism of disease to explain iron panel results (TIBC, ferritin, transferrin sat, serum iron)
- Sideroblastic anemia – using the mechanism, explain what the iron panel results would be?
Ready to start?
What is the major function of RBCs?
Carry O2 to tissues
What ion allows for O2 to bind to hemoglobin? What is the oxidation state?
O2 binds to iron ions (Fe2+)
What molecule is this iron a part of?
Heme
What is methemoglobin? What is the problem with having too much methemoglobin?
Hemoglobin, with Fe3+ instead of Fe2+; Fe3+ binds O2 very poorly
What is MCV (mean corpuscular volume)?
Average volume per RBC (in femtoliters, fL)
What is the difference between hemoglobin and heme? Which actually binds O2?
Heme is a porphyrin based MOLECULE that contains iron. The iron itself binds O2.
Hemoglobin is a protein composed of 4 globin protein subunits, each containing 1 heme molecule.
What is anemia?
Insufficient RBC number, or hemoglobin quantity
What is a microcytic anemia? A normocytic anemia?
Microcytic anemia = anemia where each RBC is too small (too little volume).
In a normocytic anemia, each RBC is “normal” in size.
So what would a macrocytic anemia be?
Anemia where each RBC is too large
Microcytic anemias – what are the MCV (mean corpuscular volume) values associated with it? Generally speaking, what will cause a microcytic anemia?
MCV < 80 = microcytic anemia Anything that decreases hemoglobin levels → microcytic anemia Think of RBC as a big balloon full of hemoglobin. If there is less hemoglobin, the balloon will be less full.
Normocytic anemias – what are the MCV values associated with it? Generally speaking, what will cause a normocytic anemia?
MCV 80-100 = normocytic anemia Anything that that affects RBC NUMBER → normocytic anemia
Macrocytic anemias – what are the MCV values associated with it? Generally speaking, what will cause a macrocytic anemia?
MCV >100 = macrocytic anemia
Anything that diminishes DNA synthesis
The way to think about it is that during RBC development, as the RBC “balloons” are filling with the hemoglobin protein, if DNA replication is too slow because there are too few nucleotides, then the RBCs will become “overfilled”
Thalassemias - generally speaking, what is the defect?
Globin chain synthesis defect (recall that globin is the protein subunit that contains heme, the iron-containing porphyrin molecule that binds O2
We will discuss elsewhere the thalassemias, and how their underlying defect explains what you see on hemoglobin electrophoresis
Thalassemias - using the underlying defect, explain what kind of anemia it would cause (microcytic, normocytic, macrocytic). Why does this make sense?
Microcytic. It is a defect in synthesizing globin, which is a component of hemoglobin. Globin ↓ → hemoglobin ↓ → MCV ↓
In other words, the RBC “balloon” is less full of hemoglobin, so the volume of each RBC will be less
What kind of anemia (microcytic, macrocytic, normocytic) would iron-deficiency anemia lead to? Why?
Microcytic anemia – need iron to make heme, so iron ↓ → hemoglobin ↓
Hydroxyurea - what is the mechanism of action?
inhibits ribonucleotide reductase (converts ribonucleotides → deoxyribonucleotides) → inhibit DNA synthesis
What kind of anemia (microcytic, macrocytic, normocytic) would hydroxyurea lead to? Why?
Macrocytic anemia – inhibits DNA synthesis
What kind of anemia (microcytic, macrocytic, normocytic) would B12-deficiency anemia lead to? Why?
Macrocytic anemia – need B12 for DNA synthesis → will take longer to make DNA, so cell will grow for longer
Don’t worry – you won’t have to memorize all of this!
I know this is a lot of information
Think about how wonderful it will feel when you open your exam results!
What are the components of an iron panel? (4)
Ferritin
Serum iron
TIBC (total iron binding capacity)
Transferrin saturation
Serum iron
TIBC (total iron binding capacity)
Transferrin saturation
What is the function of ferritin? What do we use it for diagnostically?
Ferritin – storage form of iron (in bone-marrow macrophages)
Ferritin levels in the blood correlate with ferritin levels in your body (i.e. the total amount of stored iron)
What is the function of transferrin? What do we use transferrin saturation for diagnostically?
Transferrin – iron carrier in the blood
Transferrin saturation levels are higher when iron levels are higher
What is the difference between “transferrin” and “transferrin saturation”?
Transferrin = molecule that carries iron in the blood
Transferrin saturation = % of transferring bound to iron
(analogous to hemoglobin saturation, which is the % of total hemoglobin that is bound to O2)
What will transferrin saturation generally correlate with?
Serum iron levels (i.e. if serum iron levels ↑, then transferring saturation ↑)
Ferroportin – what is its function in the body? (2)
Transport of iron into the blood from: intestinal epithelial cells, and bone marrow macrophages
What is hepcidin? What does it lead to?
Major regulator of iron absorption, and regulates iron release from bone marrow macrophages
CAUSES FERROPORTIN TO BE INTERNALIZED/DEGRADED
For clarity, I will include previous definitions for reference:
Transferrin = molecule that carries iron in the blood
Transferrin saturation = % of transferring bound to iron
(analogous to hemoglobin saturation, which is the % of total hemoglobin that is bound to O2)
Ferroportin – Transport of iron into the blood from: intestinal epithelial cells, and bone marrow macrophages
If I degrade ferroportin, what will be the effects on iron absorption in my body? Why?
Iron absorption ↓
Ferroportin allows for iron absorption into my blood stream, so if I degrade the protein → less iron absorption
If I degrade ferroportin, what will be the effects on release of iron stored in bone marrow macrophages? Why?
Iron release ↓
Ferroportin allows for bone marrow macrophage iron release, thus hepcidin → ↓ iron release from bone marrow macrophages
What causes release of hepcidin?
IL-6 (causes release of acute phase reactant proteins; produced in inflammatory states) → hepcidin production
What determines TIBC (total iron binding capacity)? What is the relationship between TIBC and ferritin (positive correlation, negative correlation, no correlation)?
TIBC correlates to the total amount of transferrin in the blood (i.e. because transferrin carries iron, the more transferrin there is, the more capacity to carry iron my blood has)
There is a NEGATIVE correlation between TIBC and ferritin. The way you can think about this is high TIBC indicates your body is “looking for iron.” In other words, if iron stores are low, it makes sense that your TIBC/transferrin would be high, since in cases of low stores of iron, your body would be trying to “find” iron.
Hepcidin – Why would it make sense that a molecule like this would exist? Why does this relationship between TIBC/transferrin and ferritin make sense?
If I have high hepcidin levels (e.g. in infection) → want to sequester iron from iron-loving bacteria, which need iron for their growth. If I’m preventing release of iron, and maintaining high ferritin stores in an inflammatory state, it would make sense that I would then want to decrease the total amount of iron transport protein in my blood. Or, using our previous example, if our iron stores are high, our body isn’t looking for iron.
Anemia of chronic disease – what is the mechanism?
It is a problem of too little iron absorption, and too little release from iron stores
Chronic inflammation → chronic IL-6 production → chronic hepcidin production → iron absorption ↓, release of iron from stores ↓
→ insufficient iron for adequate heme production → hemoglobin ↓
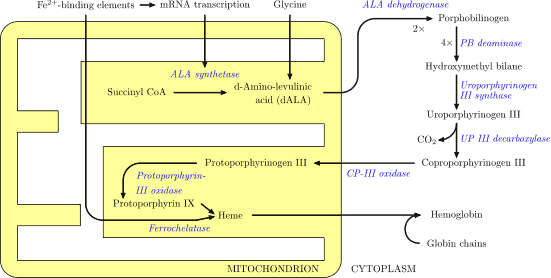
Sideroblastic anemia – what is the mechanism of disease?
Defect in heme synthesis
Wait!
I strongly recommend that you attempt to answer the final questions by yourself first, before looking at the answers. Remember, the USMLE Step 1 exam will test your ability to make connections on the spot. The more practice you have, the higher your score! Then, when you think you might know the answer (or are completely stumped), look at the answers below!
Ready for the answers?
Iron-deficiency anemia – use mechanism of disease to explain iron panel results (TIBC, ferritin, transferrin sat, serum iron)
Too little iron → serum iron, transferrin saturation ↓. Additionally, ferritin would be ↓ → TIBC ↑ (transferrin and ferritin = negatively correlated)
Anemia of chronic disease – use mechanism of disease to explain iron panel results (TIBC, ferritin, transferrin sat, serum iron)
Chronic inflammatory source (e.g. autoimmune disease) → chronic IL-6 production → hepcidin elevation → ferroportin degradation → iron absorption ↓, iron trapped in bone marrow macrophages → serum iron, transferrin saturation ↓Thus far, it is similar to iron-deficiency anemia. However, since iron is trapped inside bone marrow macrophages → ferritin ↑ and TIBC ↓, since transferrin and ferritin are negatively correlated
Sideroblastic anemia – using the mechanism, explain what the iron panel results would be?
Sideroblastic anemia = heme synthesis problem → MCV ↓, and less iron used to make heme.
However, there are no issues with iron absorption. Thus, serum iron levels / transferrin saturation would be ↑, as would ferritin. Ferritin ↑ → TIBC ↓
What should you do next?
- Turn the narrative, “Pathogenesis to Presentation” questions into Anki cards by copy/pasting the question/answer into the “Front” and “Back” fields in Anki. Do the same for the fundamental facts that you were unfamiliar with, to maximize your chances of USMLE Step 1 success! Remember: the USMLE is a test of understanding, so the better you can understand these questions, the better your score!
- Add reverse cards when appropriate to your Anki cards
- Re-word the questions/explanations as desired, and BOLD the important text to make it easier to review in the future
- Learn something new? Something unclear? Comment below!
- If you liked this post, please consider sharing it on Facebook/Twitter! I judge the utility of these posts by the number of comments / shares they receive, so if you’d like more, or would like a particular topic addressed, please let us know!
Photo from Wikimedia Commons.




{kind=link}
What’s “Pathogenesis to Presentation”? Where do I find it? …or is it your anemia questions here?
Great question – I address how to learn in a pathogenesis to presentation manner here: https://www.yousmle.com/nail-fundamentals-usmle-step-1-nbme-practice-exams/
Hi
I just wanted to let you know that I really enjoyed reading your questions.
Awesome – thanks for the feedback!!
Goodness finally someone explains it.
Thanks for the positive feedback John! Be sure to check out the other articles, and let me know how better I can help!!